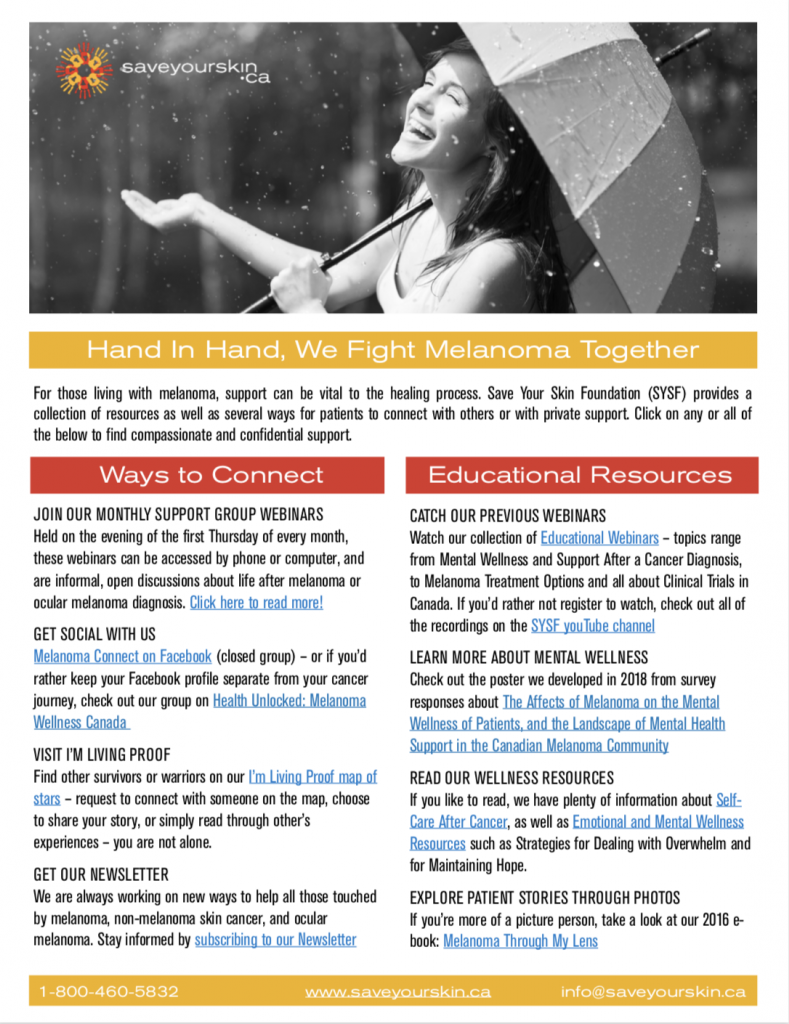
Everyone has different support needs, especially in the context of a melanoma, ocular melanoma, or non-melanoma skin cancer diagnosis. Whether you are looking for community, information, or strategies for self-care, we have resources available for you. We encourage you to take a look through our website to find what works for you, but for now, here is an overview of what we have to offer. If you are particularly looking for information and support related to the COVID-19 pandemic, you should check out our COVID-19 information hub.
In our 2017 survey report, “The Affects of Melanoma on the Mental Wellness of Patients, and the Landscape of Mental Health Support in the Canadian Melanoma Community,” Save Your Skin found that the effects of a melanoma diagnosis on the mental wellness of a patient is a real and urgent concern. Survey participants reported needing support with fear, grief, end-of-life planning, their diagnosis, next steps, living with cancer, family support, survivorship, and hope. The most ideal forms of support for participants, according to the survey, are group therapy, one-on-one therapy, and family support. The majority of participants (66% in our English survey and 84.21% in our French survey) reported wanting mental wellness support after their cancer diagnosis. Therefore, if you are fighting cancer or know someone who is, it might be helpful to participate in or share the resources below!
Webinars
Save Your Skin has been running webinars on medical and patient support topics since 2015, the video and audio recordings of which are archived on our website. These webinars are not only an excellent educational resource, but are great for connecting with the oncology community and meeting other patients and survivors. In terms of mental health support and community, the “Mental Wellness & Support After a Cancer Diagnosis,” “Living Beyond Cancer,” and “Surviving Melanoma: A Discussion on Survivorship” might be especially interesting to you– however, it is definitely worth looking through the entire list!
Patient Support Group Chats
On the first Thursday of every month, we host our informal Patient Support Group Chats. These meetings are free, can be joined by phone or online, and are open to melanoma, ocular melanoma, and non-melanoma skin cancer patients and survivors. These group discussions include patients and survivors from across Canada, and members of the Save Your Skin team, including Founder Kathy Barnard.
In addition to our support group, you can find a list of other support group options on our Additional Resources & Support Groups page, which may include something that is more local for you.
Emotional and Mental Wellness Resources Page
Our Emotional and Mental Wellness Resources page features many resources related to mental wellness. These include guides for coping with overwhelm, catastrophic thinking, and grief, for improving your quality of life, and for maintaining support networks and hope. This page also includes a link to Psychology Today’s chronic illness therapist search engine, which will help you find options for therapy in your area. On this page, you can also view our guide to self care after a cancer diagnosis.
Community and Hope
If you are looking to make connections with people who have gone through a melanoma, ocular melanoma, or non-melanoma skin cancer diagnosis, or to read stories of hope, you might also be interested in our survivorship initiatives, such as Melanoma Through my Lens, which features the stories of six Canadian melanoma survivors, or I’m Living Proof, a global map that showcases the stories of many melanoma, ocular melanoma, and non-melanoma skin cancer survivors. If you are interested in speaking to someone you see on I’m Living Proof, you can request to connect with them to be put in touch.
We hope that Save Your Skin has something to support your mental wellness, wherever you are in your journey. This Melanoma Awareness Month, consider taking the time to investigate what resources may help you, or share the graphic below to your community, as you never know who might need help. Remember: hand in hand, we fight skin cancer together.




 Saskatoon, Saskatchewan
Saskatoon, Saskatchewan Abbotsford, B.C.
Abbotsford, B.C. St. Albert, AB
St. Albert, AB

 Toronto, ON
Toronto, ON